Mr Ponosh and Ponosh Vascular provides a comprehensive diagnostic and treatment management solution to all vascular disorders.
Utilizing up to date and cutting edge, evidence based management, Mr Ponosh will tailor your treatment for the very best outcome through conservative medical therapies, minimally invasive endovascular (keyhole) treatments or open surgical operations.
Please see below for information relating to some some commonly treated conditions and treatments.
Ponosh Vascular provides the very latest, up to date and comprehensive diagnostic and management service of all vascular conditions. Utilizing the optimal conservative medical therapies, minimally invasive endovascular techniques and contemporary surgical options, we specialise in:
Peripheral arterial disease (PAD) is a condition where the arteries become narrowed or blocked by fatty deposits called atherosclerosis, more commonly known as “hardening of the arteries”.
Whilst this can occur in many arteries in your body, significant problems may arise when this narrowing causes an arterial blockage in the leg.

Over the years, cholesterol and calcium build up inside the arteries causing the narrowings. These arterial blockages occur much earlier in people who have these risk factors.
PAD has the capacity to progress from simple narrowings without many symptoms to conditions that pose increased threats to your legs.

People with any of these conditions need management of all their risk factors as underlying PAD suggests a higher risk of stroke or heart attack.
If you have any of the above symptoms or are concerned that you do, please see your General Practitioner in the first instance. They may be able to clarify other possible diagnoses but if they are concerned, they will refer you to a Vascular & Endovascular Surgeon, such as Mr Ponosh.
Whilst walking pain or claudication may limit your lifestyle, it may not require an urgent review, however if you have rest pain or a non-healing ulcer, an urgent review is essential.
Your GP may contact Mr Ponosh’s office directly, however in some cases they will provide you a referral to contact the office yourself. Mr Ponosh’s caring and helpful staff will walk you through the process of making an appointment with Mr Ponosh. His staff may also contact you directly. For further information regarding referrals, click here.
When you see Mr Ponosh, he will undertake a full history and appropriate examination. In many instances (if required), he will order appropriate tests before he sees you to streamline your management and avoid unnecessary appointments. These tests are bulk billed at all times if possible. These tests may include ultrasounds, CT scans or blood tests. In some cases, additional tests and appointments may be required.
Based upon Mr Ponosh’s expert review, an appropriate treatment plan will be suggested and explained to you in an open, straight-forward, jargon-free manner with all options and questions addressed.
If you have any questions, please do not hesitate to contact our friendly team on (08) 9386 6200.
In many cases, aggressive treatment is not required. In many patients, where there is a minimal lifestyle impact or minimal symptoms, no treatment beyond treating the underlying risk factors that cause the PAD is needed.
In mild symptoms, an active exercise program and risk factor treatment has been shown to have some benefits in improving outcomes especially in those with claudication. Dr Ponosh will discuss this with you if appropriate.
However, treatment is appropriate if you develop:
Treatment is different for every patient and depends on multiple factors including; underlying symptoms, nature of your disease, your age and underlying health issues, medications and expected outcomes for you. These treatment options range from minimally invasive procedures to open surgery for more severe conditions. Mr Ponosh takes all these factors as well as his vast personal experience and evidence-based practice to tailor the most optimal treatment for you at the lowest risk and with the best outcome. Your treatment may include one or a combination of the below options.
This means a “watch and wait” approach. As described above, if your PAD is only mild, treatment is not always in your best interests and may not always have the best outcome for you. In these cases, Mr Ponosh in conjunction with your GP and occasionally other specialists such as diabetic or heart specialists (if required) will manage you risk factors improving your long-term outcomes.
Other options such as a walking program may also be discussed with you.
Beyond the medications used to treat your risk factors and some blood thinners like aspirin, there are no other medications shown to make a “real-life” difference in your PAD.
Mr Ponosh may suggest regular review (often annually) to keep a close eye on your PAD. Of course, is you develop any concern’s or worsening symptoms, please contact Mr Ponosh’s office.
Endovascular or “keyhole” angioplasty treatments are minimally invasive procedures that usually require a day-stay or a short overnight stay. They are undertaken with an anaesthetist usually done under a local anaesthetic with sedation providing a “twilight” anaesthetic. Endovascular surgery and procedures are undertaken through a small needle access through your groin directly into your arteries. They are low risk, essentially pain-free procedures which utilise state of the art modern technologies for excellent outcomes. The results are almost immediate and have a very rapid return to your normal lifestyle.
These procedures allow Mr Ponosh to undertake a diagnostic angiogram to further assess your PAD, and in most cases, proceed to the below procedures during the angiogram to treat and cure your disease:


Balloon Angioplasty Stenting
Please see the section it “What We Do” for information on angioplasty & stenting as well as the video’s in the “Patient” section to see how stenting is done.
For a printable patient information sheet on endovascular intervention click here.
These are more invasive procedures done through larger open incisions, often under a general or spinal anaesthetic.
Open surgical options may be utilised for more complicated or extensive disease or in some cases where it has been shown to provide the best outcome.
These procedures, whilst shown to be safe and durable, have different and often higher risks than endovascular treatments and are thus only used when appropriate. These procedures may include a bypass operation in which your own vein or a plastic tube is used to bypass the blockage in your artery or an endarterectomy where a more localised blockage is surgically removed.
These procedures often need a 1-night intensive care stay with a 5-7 day stay in hospital. Mr Ponosh would discuss these procedures with you at length.

An angiogram is a procedure to visualize the flow through your arteries and identify disease for treatment. Whilst Mr Ponosh will organize ultrasounds, CT or MRI scans to assess and diagnose your vascular disease, an angiogram may be required for further information or to ultimately treat your arterial disease. In some cases, these procedures can also be used to treat your veins (venogram).
Endovascular or “key hole” angiogram treatments are minimally invasive procedures that usually require a day-stay or a short overnight stay. They are undertaken with an anaesthetist usually done under a local anaesthetic with sedation providing a “twilight” anaesthetic.
Endovascular procedures are undertaken through a small needle access through your groin directly into your arteries. Dye is injected through the needle or access tube (sheath) to show the flow through your arteries and is shown by x-rays taken during the procedure to confirm the narrowing’s or other disease that needs to be treated. The procedure takes between 45-60 minutes in most cases.

Small angiogram sheath (2-3mm) that key hole procedure is performed through.
They are low risk, essentially pain-free procedures which utilize state of the art modern technologies for excellent outcomes. The results are almost immediate and have a very rapid return to your normal lifestyle.
Preparation for the angiogram
The procedure will have been discussed at length with Mr Ponosh in his office. Mr Ponosh will the procedure to you in an open, straight-forward, jargon-free manner with all options and questions addressed. The benefits and the risks will also be discussed. A consent or permission form will be signed by you and Mr Ponosh.
You will be admitted to the hospital for a few hours in advance of your procedure to prepare for the angiogram. Mr Ponosh’s staff will confirm these times in writing with you and provide clear information on eating, drinking and fasting times. Advice will also be provided by Mr Ponosh and his staff regarding your medications. This will particularly apply to any blood thinners or diabetic medications.
Continue all your usual medications. Please advise the rooms on 9386 6200 if you are on any of the following medications :
The anaesthetist will usually contact you in the days before your procedure for further information.
During this preparation time in hospital, if you have any worries or queries do not be afraid to ask. It is necessary to put on a hospital gown and usually the hair at the groin area needs to be trimmed before the angiogram. The procedure will take place in area known as an Angiography Suite. This is like an operating theatre however it is specialized for angiograms and has additional equipment including the special x-ray machines.

Mr Ponosh with Hollywood Hospitals new state of the art, Siemens Pheno Angiography Suite.
The anaesthetist will place a small drip in your hand or arm and start your “twilight” anaesthetic. You will be positioned on the procedure table and your groin skin will be cleaned to prevent infection. The cleaning preparation is often a little cold. You will be then covered with sterile drapes. Occasionally your face will be covered but a “tent” will be made to make you feel comfortable. You will be asked to lay as still as possible however if any concerns or questions arise, the nursing and anaesthetic staff will assist you. You may feel some pushing and pressure in your groin, however the procedure should be as discomfort-free as possible.
During the angiogram
Mr Ponosh will inject a local anaesthetic into the skin at the groin numbing the area. Then the fine tube (sheath) is inserted into the vessel. With the help of wires other small long tubes called catheters can be maneuvered through the blood vessels and positioned as desired. X-ray pictures are taken whilst dye is injected down the catheter into the blood vessels. The dye may cause a hot flush and the feeling of having to pass urine. Both will subside after a few seconds. Multiple injections are necessary to see the full length of the blood vessel and the x-ray machine or the table will be moved in-between them. Mr Ponosh will identify the diseased arteries and treat your disease using either :
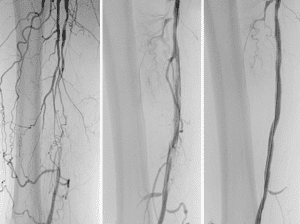
Angiogram showing blocked thigh artery (left) and re-opened (right).
Angioplasty
Some narrowed arteries (and rarely veins) are treated by passing a balloon across the diseased segment and then inflating it. The balloon will dilate the narrowing treating the blockage and improving your symptoms. The balloon is then removed. Mr Ponosh may elect to use new state of the art “drug coated” angioplasty balloons in some cases which coat the treated artery with a special drug. These special balloons have been shown to have very good long term outcomes especially in cases of re-narrowing.
Stenting
In some cases Mr Ponosh may decide a stent is the best option to treat your narrowed arteries (or vein). Stents are either a bare metal scaffold or a plastic covered metal scaffold to help hold the artery open. The use of these stents are based upon Mr Ponosh’s vast personal experience and evidence based medicine to provide you the optimal outcome. These are minimally invasive devices which are permanent and often have special drugs coating them to help improve outcomes. Please see the “Patients” section for videos showing stent insertions.
They may be used to treat narrowing or some cases aneurysm’s (blow outs or dilations) of your arteries.
Artherectomy
This is a key-hole device used in conjunction with ballooning or stenting to “drill” or excise out arterial disease. It is used in specific cases to improve outcomes.
Embolization
This is a procedure usually used on veins and occasionally arteries in which small metal coils and permanently placed in vessels to block them off. This is often used on “leaky” veins such as an ovarian vein and may be part of varicose vein treatment. The coils are made from platinum and will not cause issues with other x-rays or airport metal detectors. Mr Ponosh will discuss there use with you if required.
After Angiogram/Venogram
When the procedure is completed all access sheaths are removed from you. A special staple or plug device may be used to the small hole in your artery. Pressure will be applied to the groin for up to fifteen minutes and a small pressure device (Fem-Stop) may be placed on your groin for an hour or so. You will awaken from your twilight anaesthetic and moved to the recovery area where nurses will be keeping a close eye on you. Approximately 2-4 hours of bed rest are necessary to prevent any bleeding from the puncture site. The nursing staff will check the groin, and foot pulses at regular intervals.
Your usual medication may be adjusted after this procedure however this will be clearly detailed to you. Mr Ponosh will speak to you after your procedure and you will discuss any queries or questions with you.
You will either stay overnight or be discharged later in the day if a day case was planned. Nursing staff will keep you well looked after during your stay. Mr Ponosh’s staff will be in contact with you in the days following your procedure to arrange your follow-up in his office and any ultrasounds if required.
Click here for a printable Angiogram Discharge Information sheet for discharge advice.
Click here for a printable Patient Information Sheet on Endovascular Intervention.
Risks
An angiogram/ angioplasty is a very safe low risk procedure. Mr Ponosh has decided and discussed with you that although there are risks inherent to every procedure, the benefits to you dramatically outweigh them and the angiogram is the best treatment for you. If you have any concerns following the procedure please contact Mr Ponosh’s rooms directly, your GP, or your hospital.
Bleeding
As the operation is performed on blood vessels a small amount of bleeding can sometimes occurs. This is often easily treated with some pressure but it is common to have some bruising to the area after the procedure. You may also develop a small lump which will resolve by itself. Serious bleeding is very uncommon but may require an additional procedure to correct.
False aneurysm
Very rarely a lump may occur which is in flow with the artery. This is because of some continued bleeding from the puncture site. This is called a pseudoaneurysm. This pseudoaneurysm may settle by themselves whilst other may require an additional procedure to fix them.
Pain/Discomfort
Pain and discomfort is usually minimal during the procedure and after. Occasionally you can get some bruising and discomfort to the groin in the following days but this is minor. If you are concerned or the pain is significant please seek advise.
Allergic reactions to the dye
Very rare
Damage to blood vessels
Usually these problems can be dealt with at the time of the procedure, but in rare instances, repair is necessary.
Equipment failure
It is theoretically possible for a catheter, wire or device to break and leave a fragment inside the body. This is extremely rare.
Failure of technique
Occasionally it is not possible to perform the angioplasty or the procedure does not show the desired result. In very rare circumstances a failed procedure can actually make the blood flow worse. Catastrophic outcomes are very rare.
Kidney damage
The dye used is excreted via the kidneys, which in most patients is completely normal. However, especially in patients poor kidney function, the dye can lead to deterioration in kidney function. Angiograms are used in patients with kidney disease often and safely but additional precautions are required such as admission the night before the procedure, additional fluids and modifying your medications. Mr Ponosh will discuss these with you. Patients on dialysis do not need additional precautions and angiograms are completely safe.
Varicose veins are abnormally dilated and tortuous veins, often visible just beneath the skin. They can vary in size from quite small (1-3mm across) to very large (2-3cms across). These can be purely cosmetic or can be a sign of more significant and sinister symptoms.
Very small veins are called “thread veins” or “spider veins”. These veins are different to varicose veins because they are situated much closer or within the overlying skin. Although they may be unsightly, they are mainly a cosmetic issue and are often more challenging to treat and can cause a range of symptoms and problems.


Spider Veins Varicose Veins
Veins are blood vessels that drain used blood up the leg back to the heart. There are two types of veins in your legs. The deep veins which do the bulk of the work, and the more superficial draining system.
The deep veins are larger veins deeper in the muscles that drain the majority of your legs blood back to the heart. These veins develop conditions such as deep vein thrombosis, colloquially known as “economy class syndrome”.
The skin draining system consists of 2 veins, the long saphenous vein running from the ankle to the groin on the inside of your leg and the short saphenous vein running up you calf from the Achilles to the back of your knee. These veins drain into the deep system. The malfunctioning of these veins is the common cause of varicose veins and are the focus of treatment in many cases.
These veins have no pump but rely on a system of hydraulics moving blood up the leg against gravity. When compressed, blood moves up these veins with one-way valves stopping the blood flowing back down the leg. Under certain circumstances these valves fail or become “incompetent” with blood now flowing up and down the leg. This reverse flow back down the leg causes abnormally high pressure in the veins. The veins cannot cope with this abnormally high pressure and dilate, thus causing varicose veins.

In addition, veins particularly at the ankle are “watertight” at these high pressures and thus become “leaky”. Fluid and inflammatory cells leak out causing many more sinister, non-cosmetic symptoms such as swelling, pigmentation, itching and even ulcers. This is known as chronic venous hypertension.
Varicose veins are associated with:
Varicose veins can cause:
Please click on the below video link to hear Mr Ponosh discuss varicose veins.
This is generally a personal decision for many patients, particularly if your veins are purely a cosmetic concern. If they bother you, given the low risk, minimally invasive and durable solutions are now available for treating varicose veins. In most instances, Mr Ponosh would recommend having them treated.
Veins will never improve if left alone and will only progress, so treating them in most cases makes sense.
However, if you have more complicated veins (symptoms 5-10 from above) treatment of your veins is essential to avoid more sinister outcomes.
Your GP may contact Mr Ponosh’s office directly, however in some cases they will provide you a referral to contact the office yourself. Dr Ponosh’s caring and helpful staff will walk you through the process of making an appointment with Mr Ponosh. His staff may also contact you directly. For further information please regarding referrals, click here.
When you see Dr Ponosh, he will undertake a full history and appropriate examination. In many instances (if required), he will order appropriate tests before he sees you to streamline your management and avoid unnecessary appointments. These tests are bulk billed at all times if possible. These tests most commonly include an ultrasound of your legs and occasionally your abdomen. In some cases, additional tests and appointments may be required.
Based upon Mr Ponosh’s expert review, an appropriate treatment plan for your best long term outcome will be suggested and explained to you in an open, straight-forward, jargon-free manner with all options and questions addressed.
If you have any questions, please do not hesitate to contact our friendly team on (08) 9386 6200.
Treatment is not “one size fits all” especially when it comes to varicose veins.
Mr Ponosh if one of the few vascular specialists in Perth to provide a truly comprehensive management service for varicose veins, offering all the up-to-date available therapies to tailor your treatment for the best outcome. The cosmetic varicose veins treatment options range from non-invasive or minimally invasive procedures, such as sclerotherapy (injection therapy), laser vein removal or radiofrequency ablation, to modern varicose vein surgery options. Mr Ponosh’s experience of treating veins extends into the thousands over many years.
Our service is not a matter of “square peg for a round hole” like others do but finding the correct round peg for that round hole.
Options are different for every patient and depends on multiple factors including; underlying symptoms, nature of your disease, your age and underlying health issues, medications and expected outcomes for you. Mr Ponosh takes all these factors as well as his vast personal experience and evidence-based practice to tailor the most optimal treatment for you at the lowest risk and with the best outcome.
Your treatment may include one or a combination of the below options.
These include wearing compression stockings, elevation, and exercise.
Radiofrequency Ablation (RFA) or Laser Vein Ablation (EVLT)
This is a more modern and minimally invasive varicose vein treatment. It is designed to be a “walk in walk out” procedure, so you can leave on the same day. It is conducted in our rooms under local anaesthetic with excellent long-term outcomes.
Click here see additional information about endovenous ablation
Click here for a printable Patient Information Sheet on endovenous ablation
Injection Sclerotherapy
This is used in all types of varicose veins and a microinjection technique may be used for thread veins. It is a simple, low risk and non-invasive vein treatment.
However, it may not be as effective as other techniques for larger varicose veins especially if there is a major draining vein malfunction.
Click here see additional information on sclerotherapy
Click here for a printable Patient Information Sheet on Sclerotherapy
Topical Excel V+ Laser Therapy
Ponosh Vascular has recently acquired the latest and most comprehensive topical laser system available. The Cutera Excel V+ laser system allows us to treat spider veins beyond the scope of sclerotherapy with amazing results as well as other conditions such as port wine stains, benign pigmented skin spots, rosacea as well as a number of cosmetic treatments.
Click here see additional information on topical laser therapy
Click here for a printable Patient Information Sheet on topical laser therapy
Cosmetic surgery for varicose veins is still a common form of treatment and an effective way of removing veins. Techniques have changed over the years with excellent outcomes and shortened recovery.
Click here see additional information on vein surgery
Click here for a printable Patient Information Sheet on vein surgery.
What is Carotid Artery Disease?
Arteries throughout the body can become narrowed or even occluded (blocked) by a build up of cholesterol, fat and calcium known as an atherosclerotic plaque. This can occur to the carotid arteries that supply blood to your brain.
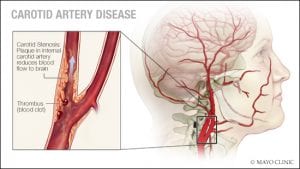
The brain is supplied by two large carotid arteries (right and left) which supply the front two thirds of your brain. These carotid arteries pass up each side of the neck and divide into internal and external carotid arteries. The internal carotid arteries supply oxygen-rich blood to your brain. The external carotid arteries supply oxygen-rich blood to your face, scalp, and neck. It is the of the narrowing internal carotid artery that is of concern as it supplies the brain itself, especially critical areas that are associated with vision, movement & sensation to your face, arms and legs as well as speech. These internal carotid arteries are often treated for severe narrowing.
The back third of the brain is supplied by two smaller arteries known as vertebral arteries. These form a complicated network of arteries with the internal carotid arteries known as the Circle of Willis inside the base of your skull. These vertebra arteries are only very rarely associated with significant symptoms are rarely need treatment.
The narrowing of the internal carotid arteries in many case be associated with no symptoms at all and can be called asymptomatic. However in some instances can cause :
What causes Carotid Artery Disease?
Lifestyle conditions are mostly to blame for the damage caused to the arteries.
Major factors that contribute to this damage include:
These conditions cause damage to the walls of arteries and as part of the healing process, atherosclerotic plaques form which cause narrowing of the arteries.
Suprisingly it is not the reduction of flow in the carotid artery that causes strokes or other symptoms in most instances but is in fact small microscopic particles that dislodge from the plaque that travels to the brain (emboli), blocks the microscopic blood supply causing an area of brain to die. This is what a strokes or mini-strokes is.
Studies have shown the severity of stenosis is a defacto measure of the risk of this emboli forming. Mild-moderate carotid disease is very common but largely not of a significant concern beyond closely watching it. It is the severe degrees of narrowing that pose the greatest risk.
What are the signs and symptoms of Carotid Artery Disease?
Carotid artery disease can go undetected (or be asymptomatic) until a problem develops like:

These symptoms may last up only minutes in a ministroke or may last for days-weeks or even permanently in a major stroke.
The effect of a stroke or mini-stroke may be minor but can be extremely severe or life-changing in many cases.
The brain is “cross-wired” so right carotid disease may cause left sided symptoms or visa versa. Carotid artery disease symptoms rarely effect both sides simultaneously.
Dizziness, or loss of consciousness are very rare symtoms of carotid disease.
What are the stages of Carotid Artery Disease?
Carotid Artery Disease often progresses very slowly over many years and is asymptomatic for a very long time. Once detected, CAD should be monitored on a regular basis by ultrasound and under the guidance of a Vascular Surgeon. This way, if it progresses to a point where the risk of stroke is greater than the risks associated with surgery, appropriate surgery can be performed in a timely fashion.
What should I do?
Carotid Artery Disease should not be left unassessed or unmonitored. It is best to be proactive in seeking regular checkups with your GP, especially if you are in the risk groups mentioned above. Sometimes, if you have other vascular problems, or even heart problems, your doctor will look specifically for Carotid Artery Disease during an examination, because if you have blockages in some arteries you are at increased risk of having blockages in others.
This will normally result in you being sent to have an ultrasound called a ‘Carotid Ultrasound’.
What if I don’t have my Carotid Artery Disease treated?
Some people with Carotid Artery Disease do not require intervention because it never progresses to a point where intervention is warranted.
However, everyone with significant Carotid Artery Disease should be under surveillance to monitor whether the disease is progressing or not, so that treatment can be provided when appropriate. In most cases this becomes a decision to when the risk of the narrowing causing a stroke exceeds the risks of treating it. Mr Ponosh will discuss this at length with you.
What treatment options are available?
Conservative management
If your tests suggest that the Carotid Artery Disease of low risk and the risks of treatment outweigh the benefits no treatment is required. You will need to simply monitor your symptoms and maintain regular visits with your GP and Mr Ponosh. This may change as time progresses but the vast majority of patients do not ever need treatment.
Surgery
Two main surgery methods for treating CAD are:
Carotid Endarterectomy
This is an open procedure that involves an admission into hospital and a 3-5 day stay in hospital following the procedure.
A Carotid Endarterectomy is performed under a general anaesthetic in most circumstances and usually takes approximately 2 hours.

During a Carotid Endarterectomy the surgeon makes a vertical or curved incision in the neck to expose the affected carotid artery. The aim of this procedure is to clear the buildup from inside the artery, so the surgeon will clamp the artery, make an incision and clean out the problematic plaque. The clean artery will then be closed with a hand sown ‘patch’ made from a synthetic material, and finally, the neck incision will be closed.
Carotid Stenting
Carotid Stenting is the insertion of a stent (metal scaffold) through a small incision in the groin. Special X-ray equipment and dye allow the surgeon to safely move the stent from your groin to your carotid artery in your neck.
The stent is designed to keep the artery open and to trap any plaque.

Stenting is minimally invasive, since the surgeon will only make small incisions in the groin area, rather than a larger neck incision.
The surgeon will consider very carefully whether you have disease morphology that is suitable for stenting. Stenting is usually reserved for patients who cannot undergo a Carotid Endarterectomy.
Stenting is performed under angiographic control, with a local anaesthetic and sedation and usually takes approximately 2 hours. The hospital stay and admission is similar to the Carotid Endarterectomy.
Risks of Carotid Treatment
General Risks include :
Specific Risks of Carotid Endarterectomy include :
Specific Risks of Carotid Stenting include :
After treatment
Unfortunately, Carotid Artery Disease cannot be cured, but rather, treated with surgery, adjustment of lifestyle factors and the taking of blood thinning medications. Sometimes, even with diligent following of the doctor’s instructions and good management of lifestyle factors, the disease can recur, so it is important to have ongoing surveillance with your Mr Ponosh.
This will usually involve ultrasound of the carotid arteries, along with consultation. By doing this on a regular basis, you and your doctor can identify if your disease is recurring or progressing and offer adjustments to your treatment.
An artery is a blood vessel that carries oxygen-rich blood from your heart to all the parts of the body. An aneurysm is a condition where the walls of the artery dilate or “balloon” out. This ballooning may increase in size and finally burst leading to bleeding or the artery blocking off.
Aneurysms can occur in the largest artery in your body known as the aorta in your chest or abdomen (belly) as well as more rarely in the arteries of your leg.
Click here for more information about aneurysms.
Ulcers are unfortunately a not uncommon problem that Mr Ponosh sees. They also are a very serious problem. They are a challenge to treat, and a frustration and significant disability for patients
Ulcers are open wounds, commonly to legs, ankles, feet and toes that occur spontaneously or more frequently after minor trauma such as a new pair of ill-fitting shoes.
They can be superficial or can be deep wounds with areas of skin and tissue loss. They do not heal quickly or only deteriorate, persisting for weeks or more
Causes of Ulcers
There are many causes of ulcers that cause wounds to spontaneously occur or worsen a minor injury :
How ulcers can appear
Ulcers can most commonly present as an area of skin and tissue loss. These may be small or in some cases which have been left untreated may be quite large. They can occur at areas of trauma such as the shin, or heel/toes after wearing ill fitting shoes. They can spontaneously occur over the ankles and on/in between your toes.
They may be painful, however in some cases especially if you are diabetic may be completely unnoticed and pain free. They may become infected with red, hot and swollen skin around them. Most concurringly, if they progress underlying bone and tendons can be exposed which is a very serious problem.
Ulcers can often be ignored and underappreciated by medical practitioners, however they should never be and always should be seen and managed by an expert such as Mr Ponosh. Most small ulcers are relatively straight-forward to fix but if they are large or complicated, they can take months to heel and are more challenging.
All ulcers with a known cause, presumed cause or risk factor or persisting for more than 2-3 weeks should be referred to a specialist wound service such a Mr Ponosh provides.
Mr Ponosh has a vast experience in managing ulcers and it is an area or particular interest. Mr Ponosh has a long history as a Senior Consultant to the Sir Charles Gairdner Foot & Leg Ulcer Clinic.
What if I don’t have my Chronic Ulcers treated?
Ulcers in most people with underlying causes will never heal by themselves.
Left untreated, ulcers will often progress and place you at risk of severe infection or even blood poisoning (septicaemia). Chronic ulcers can cause you to feel chronic pain, feel chronically ill and tired and may get in the way of your quality of life.
Ulcers may stop you proceeding to other operations such as hip or knee replacements.
Most concerningly, as these ulcers progress and expose tendon or bone, these ulcers may put toes or even your foot at risk.
Seeing Mr Ponosh
Your GP may contact Mr Ponosh’s office directly, however in some cases they will provide you a referral to contact the office yourself. Mr Ponosh’s caring and helpful staff will walk you through the process of making an appointment with Mr Ponosh. His staff may also contact you directly. For further information please regarding referrals, please go to Make an Appointment.
When you see Mr Ponosh, he will undertake a full history and appropriate examination. In many instances (if required) he will order appropriate tests before he sees you to streamline your management and avoid unnecessary appointments. These tests are bulk-billed at all times if possible. These tests may include ultrasounds, CT scans or blood tests. In some cases, additional tests and appointments may be required.
Based upon Mr Ponosh’s expert specialized review, an appropriate treatment plan will be suggested and explained to you in an open, straight-forward, jargon-free manner with all options and questions addressed.
Treatment Options
They key to curing your ulcers is the diagnosis and treatment of underlying causes. Treating ulcers effectively also relies on a team approach which Mr Ponosh will supervise and co-ordinate. Mr Ponosh’s multidisciplinary ulcer team includes :
In most cases these treatments can be undertaken as a outpatient with Mr Ponosh managing you through his rooms but occasionally if more severe, Mr Ponosh may need to admit you to hospital for more appropriate treatment.
Treatment may include :
How long to heal my Ulcer?
Some ulcers will be relatively simple to treat over a few weeks, however other ulcers may take many weeks or months to heal even with aggressive treatment.
Patience, persistence and compliance is the key to healing these wounds.
In almost all cases we do heal the ulcer although there is the rare instance of unusual ulcers that do not heal. This is very rare.
Ulcers, especially in damaged skin such as venous ulcers do have a tendency to recur, however with Mr Ponosh’s advice, these is a very infrequent and rare outcome.
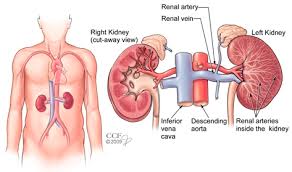
What is kidney failure?
The kidneys work as a filter to remove waste products that build up normally in the blood stream. These waste products are then passed from the kidneys to the bladder by two tubes (ureters) running from the kidneys to the bladder. The waste products are dissolved in water and stored in the bladder as urine. Kidney failure occurs when the kidneys are unable to remove waste products from the blood stream and they build up in the blood stream (uraemia).
Early on this may not be a problem, as the kidneys may continue to do some filtering work and are able to compensate for a mild degree of failure. The kidneys are able to compensate even when one of them is removed, but eventually they are unable to keep pace with the build up of waste products (chronic renal failure). If treatment is not started the patient with kidney failure will die. In these patients there is usually time to permit full discussion and planning of treatment as the kidney failure develops slowly.
Sometimes kidney failure can develop more suddenly (acute renal failure). In these circumstances there is little time to plan treatment, which must be started immediately. This may happen as an isolated problem or as part of a serious acute illness.
What treatment is available for kidney failure?
The treatment for kidney failure is dialysis. Dialysis is a way of removing the waste products from the blood stream when the kidneys cannot cope. It is like having an artificial kidney.
There are two main methods of dialysis: HAEMODIALYSIS or PERITONEAL DIALYSIS (PD).
Peritoneal dialysis involves placing a plastic tube into the abdomen and running special fluids in and out of the abdomen. The waste products dissolve in the fluid and are removed when the fluid is removed from the abdomen.
Haemodialysis is a method that requires access to the blood stream. In other words a connection between the blood stream and the artificial kidney (dialysis machine) is needed to enable this method to work. There are many ways of making this connection to the blood stream:
Central Venous Access
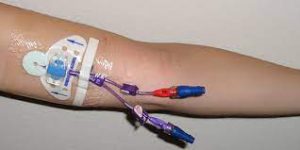
This is where a hollow tube (central line or Hickman) usually with 2 ports is placed into a main vein. They are usually placed in a main vein in the neck, but are also sometimes placed in veins in the leg. When dialysis is required the tube is connected to the dialysis machine. These tubes are in common use and are especially important for a patient who requires dialysis in an emergency. Because there is a permanent connection from the blood stream to the outside there is a risk of blood stream infections developing (septicaemia).

Creation of a fistula
A direct connection between an artery and a vein is created at a surgical operation. This new connection is called a fistula. The vein enlarges over a period of weeks because arterial blood at a higher pressure is now flowing through the vein. When dialysis is required needles are inserted into the vein and connected to a dialysis machine. Planning for the creation of a fistula should take place before dialysis is required. Patients who have a fistula in place ready for dialysis, when required, have a better chance of surviving their renal failure than patients who have no fistula.
How do fistula work?
All fistula share a common theme. The theme is the creation of a connection between a high flow, high pressure artery and a low flow, low pressure vein. This diverts blood from the artery into the vein increasing the blood flow and the pressure in the vein.
Over time the veins expand and the vein walls become much thicker (vein maturation). The time taken for the vein to mature can vary depending on which type of fistula is created. Wrist (radiocephalic fistulas) take approximately 4-6 weeks. Brachio-basilic (upper arm) fistulae take longer, approximately 8 weeks, to mature.
When the vein matures it is much easier to insert needles into the veins, as the veins are larger. The veins can also withstand repeated needle punctures over many years.

What are the different types of fistula?
There are many different types of fistula that have been devised to help patients to dialyse. Fistulae are performed in 2 major parts of the body – in the arms or in the legs. Arteriovenous fistulae created in the arm are by far the commonest type of fistula used for dialysis.
Any fistula, whether it be in the arm or the leg, can be formed in 2 ways. Firstly, the surgeon may use the native arteries and veins found in different parts of the body and, using various surgical techniques, join a vein to an artery. These are called autogenous fistulae and are always the first choice because they are likely to work for longer and need less maintenance to keep them going.
The alternative technique uses an artificial material (usually gortex (PTFE)) as a bridge between an artery and a vein. This type of operation is commonly performed at the elbow with the loop of artificial material placed in the forearm. In patients who have artificial material implanted, dialysis needles can be placed directly through the material to enable dialysis to take place. This can be a very successful technique, but in general these fistulae do not last as long as autogenous fistulae and need more maintenance procedures to keep them functioning.
Artificial materials should only be used when there is no obvious autogenous fistula that can be created or the chances of success are clearly worse than trying to use an artificial graft.
Radiocephalic wrist fistula
This is the most common fistula and is created at the wrist (primary radiocephalic fistula). A small vein (cephalic vein) and a small artery (radial artery) are joined together using very fine stitches (see below). This fistula was first devised in the mid 1960s and is still the most common fistula in use for haemodialysis.
Brachio-cephalic fistula
A brachio-cephalic fistula is formed at the front of the elbow by connecting the cephalic vein and the brachial artery at the elbow. The cephalic vein is found towards the outside of the upper arm and as it enlarges this vein can be used for dialysis.
Brachio-basilic fistula
A brachio-basilic fistula is formed at the elbow by connecting the basilic vein and the brachial artery at the elbow. The basilic vein is found on the inside of the upper arm but it is also quite deeply placed and so it needs to be transposed (moved) to a more superficial position. This involves extra incisions along the inside of the upper arm and the graft is then tunnelled in the subcutaneous tissues to enable easier access. Once a brachio-basilic fistula has been formed it is more difficult to form a brachio-cephalic fistula and so surgeons will usually attempt to create a brachio-cephalic fistula first if possible. Fortunately, if the brachio-cephalic fistula fails it is still possible to create a brachio-basilic fistula.

PTFE loops
Sometimes it is not possible to create fistulae using autogenous or native vein. In these cases an artificial plastic tube is attached to the brachial artery at the elbow and tunnelled as a U-shaped loop in the forearm or upper arm. It is then joined to a vein at the elbow and the tube itself can be used for dialysis.
PTFE may also be placed in the upper arm as a graft between the brachial artery and the axillary vein in the armpit.
Leg loops
If it is not possible to create a fistula in either arm then it may be possible to form either a vein loop or a PTFE loop in the thigh.
There are many other types of fistulae available to surgeons but they are required much less frequently than those listed above. The more unusual variations although not routinely required can be very useful in patients who have already had multiple operations to provide vascular access.
Which type of fistula is the best?
It has become clear that the best type of fistula to have created should use the native veins and arteries. Although artificial grafts can be used successfully they are usually not as useful for as long and require far more procedures, such as angioplasty, to keep them patent and useful for dialysis.
It is best to create a fistula as close to the hand as possible so that a long length of vein on the forearm and arm is available for dialysis. It is usually preferable to use the non-dominant hand (use the left wrist if the patient is right handed).
It is sometimes suggested that elderly patients are not as suitable for primary fistulae because their blood vessels may be more damaged and patency rates are not as good. This is not true. Elderly patients can benefit just as much as younger patients from primary fistulae. In patients with diabetes, wrist fistulae are much more likely to fail early but are still worth considering as a first option.
How will I be assessed before surgery?
History
The surgeon will need information about previous vein punctures (such as from taking blood or IV drips), central lines (tubes placed in large veins in the neck) and arterial lines (tubes placed usually in the radial artery at the wrist). General health information and medication will be important especially if the patient is taking warfarin which can cause bleeding.
Examination
The arms of the patient should be examined with and without a tourniquet looking for veins that may be suitable for fistulae. Scars from previous central lines, intravenous lines and arterial lines are also important. The arterial pulses in the arms should be checked.
Investigations
Sometimes a history and examination will be enough for the surgeon to decide on which operation is required. This is often the case when patients are undergoing fistula formation for the first time. There is an increasing use of imaging to help in planning the optimum surgery. Ultrasound is commonly used in the planning of your fistula.
How are fistula operations performed?
All of the operations to create a fistula require some sort of anaesthetic. Commonly, a local anaesthetic and sedation is used for most fistulae. This requires the injection of an anaesthetic under the skin which then numbs or freezes the area where the operation will be performed.
Other types of fistulae, especially prosthetic ones require a regional or general anaesthesia.
The choice of anaesthetic may be made after discussion between the surgeon, anaesthetist and patient and will also depend on which type of operation is being performed. Most operations will not take longer than 90 minutes.
How will I know if my fistula is working?
After the artery and vein have been joined together there will be a much faster blood flow in the vein. Because the join is an artificial connection, the flow is not as smooth as in normal blood vessels. Turbulence is created in the blood, much as it occurs in river water passing over rocks and boulders. This turbulence can be felt through the skin of the arm over the vein as a buzzing sensation (medically termed “a thrill”). This turbulence also creates a noise (bruit) that can be heard with a stethoscope.
If a thrill or buzz is present, your fistula is working. If it is not present your fistula may have stopped and medical help should be sought immediately.
How long will a fistula last?
How long a fistula lasts depends upon what type of operation is performed and the condition of the artery and vein before surgery. One year after surgery to create a fistula at the wrist (radiocephalic fistula) approximately 70-80% of patients will have a functioning fistula that they can use for dialysis.
Can I prolong the life of my fistula?
There are no fool proof ways of ensuring that your fistula continues to work well. Varying the needle insertion sites for dialysis may be helpful. Avoidance of blood pressure tests and blood tests from the fistula is also important.
It is important not to smoke. Loose clothing on the arms will prevent constriction of the veins. Avoid working with the arm up (eg painting a ceiling) as this can lead to compression of major veins around the shoulder and lead to thrombosis (blockage of the vein by blood clot).
If you notice any changes in the fistula they should be reported to your doctor. Changes which may be important are the buzz becoming fainter, the buzz disappearing and the fistula becoming softer. Problems with flows on dialysis or increased return pressures are also important but there appears to be no benefit for routinely monitoring flow as a screening tool for potential graft/fistula flows.
What are the possible complications from fistulae?
The fistula may block
Although most patients will leave the operating theatre with a functioning fistula and a palpable “buzz”, the main problem they are likely to run into later is that the fistula will block. The easy way to tell if a fistula has blocked is to feel the fistula. If the buzz or thrill has disappeared then it has probably blocked. If you think this has happened it is important to see a doctor immediately. Sometimes further surgery can save the fistula and keep it running, but it is often better to construct a new fistula.
Failure to mature
Sometimes the fistula may continue to work, but the vein may not enlarge sufficiently to permit its use for dialysis (failure to mature). It is not always clear why this occurs, but it usually means a new fistula will have to be created.
Vascular steal
Because blood from the artery is being diverted into a vein before it reaches the hand some patients can develop problems from shortage of blood to the hand (steal syndrome). This does not occur in most patients, but can be a serious problem if it does arise. It is very uncommon in patients who have fistulae at the wrist. It is more likely to arise when fistulae are created in bigger blood vessels aound the elbow, when it may occur in up to 10% of patients but in the majority of patients resolves without issue.
Symptoms of steal can include a cold hand, pain, discolouration and ulceration. Symptoms are typically worse on dialysis. Steal may be more likely to develop if the patients has peripheral vascular disease and/or diabetes. Before treating the steal it is important to fully investigate the cause with a fistulogram and/or an ultrasound. On some occasions an arterial narrowing proximal to the fistula can be responsible and it often easily treated with angioplasty.
If steal syndrome develops the fistula may have to be tied off to restore blood flow to the hand. This will solve the steal but the fistula will then be lost. Sometimes other procedures are available to improve blood flow and at the same time to preserve the fistula. These procedures include banding, interposition grafting and the DRIL (distal revascularisation and interval ligation) procedure. Interposition grafting with a tapered synthetic graft can be effective and has the advantages that normal arteries are left intact. It is essentially a more controlled form of banding.
Vein narrowing
In some patients narrow portions (stenosis) can develop in the vein. These may cause reduced flow in the fistula or high return pressures when the patient is on dialysis. The fistula thrill may reduce and the fistula may become noticeably softer. When this happens further investigations are required such as ultrasound scans or a fistulogram. A fistulogram involves placing a needle into the vein and injecting a dye to obtain an outline of the fistula when an X-ray is taken. Narrow sections of a fistula can either be treated by angioplasty, stenting or surgery to open up the narrowing.
Treating a venous outflow narrowing appears to be best performed with a stent-graft rather than just simple angioplasty. Longer term outcomes will be important to monitor.
Other complications
Small and even large aneurysms can develop in the veins. These sometimes require treatment but are often left alone unless they become very large.
Synthetic grafts can develop infection from multiple punctures and this can be a serious problem which requires removal of the graft and loss of the fistula.
Peritoneal dialysis is a treatment for kidney failure that uses the lining of your abdomen, or belly, to filter your blood inside your body. Doctors call this lining the peritoneum. It is undertaken through a soft tube, called a catheter, in your belly a few weeks before you start treatment. The tube is left exposed allowing you to commence dialysis.

The choice of dialysis is usually made by you and your kidney specialist. Mr Ponosh is directed by your kidney specialist. In some cases a fistula and a peritoneal dialysis catheter may be requested. Peritoneal dialysis has the advantage of allowing you to lead a more active lifestyle as the process can be conducted at home, although it does rely more on you to undertake the process
You will have extensive education and follow-up support by the dialysis teams co-ordinated by your kidney specialist so do not worry or be s.cared about taking control of your own dialysis
When you start peritoneal dialysis, dialysis solution—water with salt and other additives—flows from a bag through the catheter into your belly. When the bag is empty, you can disconnect your catheter from the bag and cap it so you can move around and do your normal activities. While the dialysis solution is inside your belly, it soaks up wastes and extra fluid from your body. After a few hours, you drain the used dialysis solution into a drain bag. You can then dispose of the used dialysis solution, which is now full of wastes and extra fluid, in a toilet or down the drain of a sink or bathtub. Then you start over with a fresh bag of dialysis solution.
The process of first draining the used dialysis solution and then replacing it with fresh solution is called an exchange. Most people do four to six exchanges every day, or during the night using a machine that moves the fluid in and out. The process goes on continuously, so you always have dialysis solution in your belly soaking up wastes and extra fluid from your body.
Peritoneal dialysis tubes are inserted by Mr Ponosh. They are usually undertaken under a brief general anaesthetic through a small incision near your belly button. They require an overnight stay and you will return to normal activities over a few days.
The risks of this procedure include :
What is Renal or Mesenteric Disease?
Renal (Kidney) and Mesenteric (bowel) arterial disease is a condition caused due to hardening and narrowing of the arteries to the kidneys or bowel. Normally, your arteries are smooth and unobstructed on the inside but a collection of fats, cholesterol and calcium can build up forming a ‘plaque’ builds up in the artery walls. This process is called as atherosclerosis, or hardening of the arteries. Formation of these plaques in the renal and mesenteric arteries will restrict the blood flow (stenosis) in the arteries.
Renal Arterial Disease
The kidneys perform functions such as removal of body waste in the form of urine, and regulation of the blood pressure by secreting a hormone, renin. If the kidney arteries are narrowed or have a clot, the kidneys will not function properly causing your blood pressure to rise which will further lead to kidney failure. These narrowing’s can cause deterioration in your renal function over time that may not be recoverable.
Renal artery stenosis may not have any symptoms. The disease develops slowly. The first sign of renal artery stenosis if you have high blood pressure is worsening of the high blood pressure or uncontrolled hypertension even with use of antihypertensive medications. Other signs include decreased kidney functions, congestive heart failure, or a small shrunken kidney. Treatment is normally reserved for extremely poorly controlled blood pressure or if there is evidence that the kidney itself is at risk.
Mesenteric Arterial Disease
The bowel, and other organs such as your liver and spleen are provided blood via three arteries that arise off your aorta, the biggest artery in your body. These three arteries are :
These three arteries form a network between each other and thus all contribute collectively. In most cases severe disease needs to occur in 2 or the 3 arteries to cause symptoms.
Mesenteric arterial disease is not uncommon but is not often treated. In most cases the narrowed arteries cause no symptoms and can be left alone. In some cases it can cause post-eating pain (known as post-prandial pain or mesenteric angina). This is severe pain that comes on after meals that lasts several hours. It is often associated with avoiding meals, loss of weight and in some cases malnutrition. It is caused by the narrowed arteries stopping enough blood getting to the bowel when needed for digestion. This is a serious and life threatening condition that needs to be treated as in some rare cases it can be so severe that it can cause sections of the bowel to die which is a catastrophic and life threatening emergency. This is a condition however that develops slowly over time. In some rare cases it can be associated with a sudden or acute event but this is associated with clot landing in these arteries associated with an irregular heart beat like atrial fibrillation or AF.
What Investigations are done to look for these conditions?
Blood tests and kidney function tests are done to evaluate the kidney functions. Other diagnostic tests such as Duplex ultrasound scan, CT scan, and angiography are done to detect the exact location of the blockage.
In some cases a review by a kidney specialist may be required.
What treatments are available for Renal & Mesenteric Disease?
The two procedures used to treat the narrowing of renal or mesenteric arteries are balloon angioplasty and stenting which are minimally invasive keyhole solutions.
Balloon angioplasty – In this technique, your surgeon inserts a catheter through a small needle which passes through the blood vessels into the renal or bowel arteries. The catheter carries a small balloon that inflates and deflates. When this is passed into the blocked artery, the balloon is inflated which will push the plaque against the artery wall helping the artery allow more space to increase the blood flow

Stenting – It is performed during an angioplasty procedure. Stent is an artificial device, a mesh-like tube which is made up of stainless-steel that has the ability to expand inside the blocked artery. Stents are mounted on narrow tube (catheter) which has a deflated balloon towards the end. This stent is inserted into the blocked artery and the balloon is inflated which allows the stent to expand inside the artery. Later the balloon is deflated and removed
Please see our information sheet above on Angiograms for further information.
Surgery – Rare and not often used due to the effectiveness of key-hole solutions.
Click here for a printable Patient Information Sheet on Endovascular Interventions
Click here for a printable Patient Information Sheet on Endovascular Discharge
Pelvic venous congestion syndrome (PVCS) is a cause of chronic pelvic pain and is a secondary cause of leg varicose veins in approximately 13-40% of women. Pelvic congestion syndrome is condition often caused by the dilatation of the ovarian or other pelvic veins, like varicose veins but in the pelvis.
However, in almost all cases, the treatment of pelvic congestion syndrome is very simple.
Varicose veins are most commonly seen in the legs. They occur due to a failure of the valves in the leg veins (see varicose vein information sheet for more details). This causes the blood to pool, causing enlarged, bulging and dilated veins. This is also what happens to the pelvic veins in PVCS. This pressure can cause a number of abdominal or pelvic complaints but can also be a cause of lower limb varicose veins and swelling, through the indirect pressurisation of leg veins.
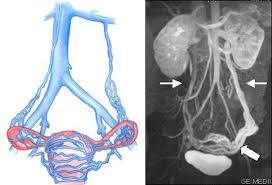
Ovarian vein incompetency (graphically and on MRI)
In men, PCVS through the malfunctioning of a testicular or gonadal vein (the male equivalent of the ovarian vein), can cause dilated veins in the testicles (varicocele), testicular discomfort, infertility and varicose veins. This is treated in a similar fashion to PCVS.
Another associated condition is May-Thurner Syndrome. This condition can cause PCVS but can more commonly cause left leg swelling and can be a cause of deep vein thrombosis (DVT). This is caused by compression of your left iliac veins by your iliac arteries causing blood to pool in your leg. Whilst a minimal degree of compression is present in all of us, in rare cases the compression is severe and needs treatment.

May Thurner Syndrome (Illiac Vein Compression by Illiac Artery)
The cause of the dilated ovarian/pelvic veins in PVCS is poorly understood. PVCS most commonly occurs in women who have had children. During pregnancy, the ovarian vein can be compressed by the enlarging womb or enlarged because of the increased blood flow. This is thought to affect the valves in the vein causing them to stop working. This causes poor pelvic drainage and pooling of blood in the pelvic veins.
There are other causes that may cause obstruction to the ovarian and pelvic veins leading to PVCS, which are much less common. It can also occur spontaneously or associated with an aberrant venous anatomy. PVCS may also be associated with polycystic ovaries. The absence of the vein valves due to abnormal development may also be a contributing factor.
The varicose veins in the pelvis surround the ovary and can also push on the bladder and rectum. This can cause the following symptoms:
Your GP may contact Dr Ponosh’s office directly, however in some cases they will provide you a referral to contact the office yourself. Dr Ponosh’s caring and helpful staff will walk you through the process of making an appointment with Dr Ponosh. His staff may also contact you directly. For further information regarding referrals, click here.
If you have any questions, please do not hesitate to contact our friendly team on (08) 9386 6200.
When you see Dr Ponosh, he will undertake a full history and appropriate examination. In cases of PCVS, the diagnosis is mainly based upon your history, symptoms and examination. In many instances, he will order appropriate tests before he sees you to streamline your management and avoid unnecessary appointments. These tests are bulk-billed. The most common tests to assist the diagnosis of PCVS may be a specialised abdominal and leg vascular ultrasound and in some cases a CT scan. In very rare cases an MRI scan may be arranged but normally only after seeing Dr Ponosh.
Based upon Dr Ponosh’s expert review, an appropriate treatment plan will be suggested and explained to you in an open, straight-forward, jargon-free manner with all options and questions addressed.
Pelvic or abdominal pain can be a common symptom, often persisting for over 6 months duration. The pain is usually on one side but can affect both sides. The pain is worse on standing, lifting, when you are tired, during pregnancy and during or after sexual intercourse. The veins are also affected by the menstrual cycle/hormones and therefore the pain can increase during the time of menstruation. The pain usually is improved by lying down.
PCVS is a significant and common cause of complicated and unusual leg vein issues.
Although ultrasound, CT and MRI may be initially used, PCVS is notoriously difficult to diagnose on imaging and in many cases is not clearly defined. This is not a failure of the test but is a reflection of the challenging and difficult assessment of the presence and function of these veins.
Even if the imaging does not clearly show evidence of PCVS, if Dr Ponosh suspects its presence from his vast clinical experience, he may recommend an Abdominal Venogram.
This is a low risk, minimally invasive procedure usually conducted as a day case in hospital under local anaesthetic and light sedation so is essentially pain free (please refer to angiogram and venogram information). In a specialised x-ray room, a small needle is placed in your groin and under x-ray guided imaging and through the injection of contrast dye, the nature of your abdominal veins and any evidence of PCVS is identified. This may appear as varicose veins in your pelvis, dilated ovarian or pelvic veins or in some cases compression of other draining veins. You will be asked to hold your breath several times and occasionally a special CT scan may be taken during your procedure (Dyna CT) for a very detailed assessment.

Incompetent left ovarian vein filling pelvic varicose veins shown on a venogram.
If PCVS is confirmed, usually through the identification of a dilated ovarian vein, Dr Ponosh will proceed to definitively treat this during the same procedure. The malfunctioning vein (usually the left but in some cases the right or both) is entered with a fine wire and tube (1 mm in size) and the vein is permanently blocked off with tiny coils in a controlled and planned fashion. This is known as “coil embolisation”. The treatment of these dilated veins stops the blood pooling in the pelvis and stops the venous congestion and hypertension that causes your symptoms.

Embolized left ovarian veins on venogram.
The venogram takes approximately 20 minutes and, if found, the “coil embolisation” takes an additional 10 minutes. The benefit of this procedure is that it is definitive. It is the only way of conclusively confirming or excluding PCVS and treating it in the same procedure. In rare instances where PCVS is not found, there is still significant clinical benefit as it definitively rules out the condition. If it is present, it is easily treated. Apart from being extremely low risk and minimally invasive, it has a rapid recovery.
In cases of May-Thurner Syndrome, a venogram is also undertaken, but if found, it is usually treated with a balloon venoplasty (stretching the vein) or placing a stent to permanently treat the narrowing. Dr Ponosh will discuss this further with you if suspected.
Dr Ponosh is a no gap provider, so there is no cost for this procedure for all private health funds.
Following the procedure, some gentle pressure is applied to your groin. You rest in bed for approximately 3 hours and you in almost all instances are home later in the day. Dr Ponosh recommends a quiet day or two at home, but the procedure has little impact on your day to day life.
Benefits
Risks
Pain following the procedure is usually minimal. A dull ache in the groin is not uncommon and well controlled with paracetamol. Following the procedure, bed rest is required for a short time and most people leave the hospital within 4 hours of the procedure.
Once discharged, you are able to resume your normal activities within the first 24-48 hours. The best advice is not to overexert yourself and avoid heavy lifting or strenuous gym work for 5-7 days.
Some people may develop an aching back or loin pain, similar to period pain for a few days following the procedure as the embolised veins completely block off. This resolves rapidly and is well controlled with regular oral pain medications.
By treating your PCVS, the pelvic varicose veins should gradually shrink away over a few weeks and your symptoms improve. As the main ovarian and pelvic veins have been embolised, if you also have any lower leg varices, these can now be treated with a reduced chance of them coming back in the future (which they have a high chance of coming back if you did not have the pelvic vein embolisation). Dr Ponosh will discuss your leg vein management in detail with you. Any symptoms that you have been having related to the varicose veins in the pelvis should also slowly improve.
Click here for a printable Patient Information Sheet on PCVS
Click here for a printable Patient Information Sheet on Endovascular Interventions
Click here for a printable Patient Information Sheet on Endovascular Discharge
Total knee replacements (TKR) are a very common procedure. Whilst the vast majority are completely successful and result in a renewed quality of life, a small minority of patient’s following a TKR have ongoing symptoms and limitations.
These can symptoms can include :
In some instances these symptoms may be related to the joint itself or other mechanical causes, however in many cases no clear cause can be found.
There is increasing evidence and literature demonstrating an alternative cause of these symptoms may be associated with abnormal blood vessels forming in the tissues surrounding your knee joint. As part of an abnormal healing process following knee surgery, new arteries can grow within and around the joint (known as the synovium). This is called “synovial neo-revascularization” (NSR).

Figure 1 : Angiographic evidence of NSR
These new blood vessels can result in :
Your Orthopaedic Surgeon would have excluded all alternate causes and when no other causes can be found, they may refer you to Mr Ponosh to investigate and treat alternate causes such as synovial neo-revascularization.
Mr Ponosh will organize a number of investigations to exclude other possible causes of pain and discomfort. These tests are bulk billed and conducted in Mr Ponosh’s rooms. They may including :
There is currently no definitive non-invasive test however available to diagnose NSR.
Conservative
In some cases even though NSR is thought to be present, Mr Ponosh and your Orthopaedic Surgeon may decide a conservative approach is best suited to you. This decision is always made after a thorough discussion with you and the reasons explained. Of course, you can always choose a conservative treatment course which may include pain killers and physiotherapy.
Geniculate Embolization
Whilst the NSR and its treatment is gaining increasing acceptance and a strong body of international evidence supporting its effectiveness and safety in post TKR chronic symptoms, it is still considered a novel and relatively new procedure. It is not widely undertaken however, the elements of the procedure are routine and well accepted vascular interventions.
The treatment for NSR is through a procedure known as a Geniculate Artery Embolization (GAE). The abnormal vessels that cause NSR arise from vessels which supply the knee and surrounding tissues known as geniculate arteries. Geniculate arteries are very small branch arteries that arise from the main arteries of your leg around your knee. GAE is a minimally invasive angiographic procedure to identify these abnormal vessels and embolize (block them). This stops inflammation, leaking and bleeding associated with NSR and hopefully reduces or resolves your symptoms.
The procedure although novel, is extremely low risk and safe. Whilst no guarantee of outcome can be made, often patients referred for consideration of GAE have exhausted all other management options and have ongoing significant disability and lifestyle impairment effective their day to day lives. In this situation, given the low risk procedure and documented successful outcomes, GAE is a worthwhile and appropriate intervention.

Figure 2 : Resolution of NSR following Embolization
The procedure :
This is because :
Risks of GAE
Bleeding
As the operation is performed on blood vessels a small amount of bleeding can sometimes occurs. This is often easily treated with some pressure but it is common to have some bruising to the area after the procedure. You may also develop a small lump which will resolve by itself. Serious bleeding is very uncommon but may require an additional procedure to correct.
False aneurysm
Very rarely a lump may occur which is in flow with the artery. This is because of some continued bleeding from the puncture site. This is called a pseudoaneurysm. This pseudoaneurysm may settle by themselves whilst other may require an additional procedure to fix them.
Pain/Discomfort
Pain and discomfort is usually minimal during the procedure and after. Occasionally you can get some bruising and discomfort to the groin in the following days but this is minor. If you are concerned or the pain is significant please seek advise.
Allergic reactions to the dye
Very rare
Damage to blood vessels
Usually these problems can be dealt with at the time of the procedure, but in rare instances, repair is necessary.
Equipment failure
It is theoretically possible for a catheter, wire or device to break and leave a fragment inside the body. This is extremely rare.
Failure of technique
Occasionally it is not possible to perform the procedure does not show the desired result. In very rare circumstances a failed procedure can actually make the blood flow worse. Catastrophic outcomes are very rare.
Kidney damage
The dye used is excreted via the kidneys, which in most patients is completely normal. However, especially in patients poor kidney function, the dye can lead to deterioration in kidney function. Angiograms are used in patients with kidney disease often and safely but additional precautions are required such as admission the night before the procedure, additional fluids and modifying your medications. Mr Ponosh will discuss these with you. Patients on dialysis do not need additional precautions and angiograms are completely safe.
3. Standard risks of general anaesthetic and regional anaesthesia
Your risk for anaesthetic will be assessed initially by Mr Ponosh, but definitively by his Specialist Anaesthetists. They will discuss the low risk in detail.
Pain post procedurally is normally minimal, managed with simple pain killers
Click here for a printable Patient Information Sheet on Geniculate Embolization.
Click here for a printable Patient Information Sheet on Endovascular Interventions
Click here for a printable Patient Information Sheet on Endovascular Discharge
The venous system is often accessed to obtain blood, administer medications, and perform other medical procedures. Usually, the peripheral veins in the arms or legs are accessed. Some procedures however require long-term or repeated access to the bloodstream which may damage the peripheral veins and cause discomfort.
What is a PICC line and how is it inserted?
A PICC line is a medium-term venous access solution. It is like a drip placed but can last up to 6 weeks (compared to 2-3 days). It has an external “drip” component with the line extending to a position near your heart. It is commonly used for long-term antibiotics avoiding the need for repeat drips. It is a low-risk procedure undertaken under x-ray guidance with an incision through a 1-2mm nick in your upper arm. It is like having a complicated drip inserted.
PICC lines are removed in the rooms on the ward like a drip at 4-6 weeks in most cases.
What is an Infusaport?
An Infusaport is a device used for long-term access to the bloodstream. This device helps to minimise patient discomfort and protect the venous system. Once in place, an Infusaport helps to deliver intravenous administration of chemotherapy or other medications, IV nutrition, blood products, as well as taking blood samples for testing. It is made of two components – the port and the catheter. The port is 2cm wide and made of metal and plastic. It has a central chamber for injections. It is placed beneath the skin, normally on the right side of the chest wall. It can be used multiple times with a specialised needle. The port can be felt and sometimes seen under the skin with nothing exposed. The catheter is a soft hollow tube which runs down the vein towards the heart.
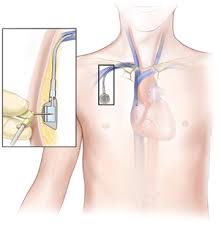

Position of port and tube Skin appearance of port under at right collarbone
The most common use for a port is for chemotherapy. The need, duration and options will be discussed with you by your oncologist or treating physician prior to the referral to Mr Ponosh.
The Infusaport can stay in indefinitely but is normally removed after treatment has finished. Removal is a minor procedure under a local anaesthetic in theatre.
How is the Infusaport inserted?
The procedure is carried out in a theatre normally under a general anaesthetic or in some cases a “twilight” anaesthesia. In most cases it is a day-case procedure.
A small pocket is then made under the skin below your collarbone through a 2cm incision. It is usually on the right side, but positioning will be dependent on your personal medical issues. The port is placed in this pocket in the chest wall. Either via the same incision or via a separate 1-2mm nick at the base of your neck, a wire is then fed along the vein and x-ray is used to check the position. The catheter is then passed down the wire into the vein and stops just above the heart. Heparin (an anticoagulant) is injected to stop any clots forming in the catheter. In some cases, a temporary needle will be left in to allow use of the port within 24-48 hours when it is still tender.
How is the Infusaport and PICC line used?
The Infusaport is accessed using a special needle (which does not damage the port’s central chamber) placed through the skin into the port. It should only be accessed by a specialist doctor or nurse trained to use this system.
A PICC line is accessed like a drip.
Possible complications.
Pain: Usually immediately after the operation, this should decrease with time.
Infection: This can be treated with antibiotics, but severe infections may result in removal of the port of PICC.
Bleeding: This can happen at the site of the operation and will normally stop if pressure is applied. Very rarely, the vessels can be damaged during the operation which is a serious complication and would require further intervention.
Blood clot in the catheter: This sometimes means a new port or PICC must be inserted but in some cases a procedure can salvage a port.
Fracture of the catheter: A rare complication, but sometimes the end of the catheter can break off and will need to be removed.
Movement of the port or catheter: This can happen even when the post is attached to the chest wall and may require revision or replacement.
Central Vein Thrombosis (Occlusion): This is a rare complication that may require the removal of the port. It is caused by the presence of the catheter, irritation from chemotherapy and the stickiness of blood cause by cancer. A PICC line can be associated with peripheral vein thrombosis or phlebitis necessitating the removal of the PICC.
Lung collapse: This occurs in less than 1% of patients having ports inserted, but occasionally the lung (pneumothorax). This normally needs a tube to reinflate the lung and prolonged stay in hospital. This can sometimes delay adjuvant treatment.
Skin problems: Occasionally there can be thinning of the skin over the port and may result in needing a new port placed in a different site.
Following your procedure.
Chemotherapy can be started the next day if needed. You can shower or bathe the next day and pat the dressing dry. Keep the wound dry for 3 days. The wound is closed with invisible stitches and glue. Remove the outer dressing after 3 days and the skin tapes will fall off over 1-2 weeks. When the skin is healed normal activities can be resumed.
In most cases further follow up is done by your referring physician unless any of the below occur.
Contact Mr Ponosh’s rooms or see your GP if you have any concerns regarding:
Click here for a printable patient information sheet on Infusaports & PICC lines.
An inferior vena cava (IVC) filter is a small device that can stop blood clots from going up into the lungs causing a pulmonary embolism (PE). The inferior vena cava is a large vein running through your abdomen (belly) into your chest, heart and lungs. The (usually temporary) device is put in during a short procedure to prevent these clots
Veins are the blood vessels that bring oxygen-poor blood and waste products back to the heart. Arteries are the blood vessels that bring oxygen-rich blood and nutrients to the body. A deep vein thrombosis (DVT) is a blood clot that forms in a vein deep inside the body. A clot occurs when blood thickens and clumps together. In most cases, this clot forms inside one of the deep veins of the thigh or lower leg.
DVT is a serious medical condition that can cause swelling, pain, and tenderness in your leg. In some cases, a deep clot in a leg vein can break free and travel to the lungs. This can cause a blockage in the vessel called a pulmonary embolism. Pulmonary embolism can cause severe shortness of breath and even sudden death.
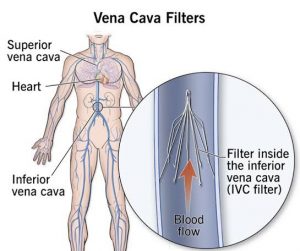
An IVC filter is one method to help prevent pulmonary embolism. Your inferior vena cava (IVC) is the major vein that brings oxygen-poor blood from the lower body back to the heart. The heart then pumps the blood to the lungs to pick up oxygen. An IVC filter is a small, wiry device. When the filter is placed in your IVC, the blood flows past the filter. The filter catches blood clots and stops them from moving up to the heart and lungs. This helps to prevent a major, life threatening pulmonary embolism.
It’s important to understand that an IVC filters does not protect against DVT. You may still get a DVT. The filter helps to protect you from a life-threatening pulmonary embolism if you have a DVT.
Mr Ponosh is normally requested to discuss and undertake an IVC filter implantation or implantation at the request of one of your treating specialists such as a haematologist, physician or surgeon.
You might need an IVC filter if you have a DVT or pulmonary embolism, or have had either of these in the past. You might need an IVC filter if you have a high risk of getting a DVT. Anything that slows the movement of blood through your veins increases your risk of DVT. A variety of conditions can increase your chance of getting a DVT, such as:
Anticoagulant (blood thinning) medication such as warfarin, clexane or apixaban are also used to treat people who are at risk of pulmonary embolism. Blood thinners may be used alone to prevent pulmonary embolism. But in some cases, they may be used along with the IVC filter.
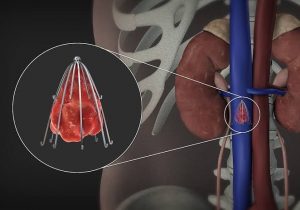
Indications for an IVC filter :
The IVC filter is placed through a small incision in a vein in your groin, conducted usually as a day case procedure with X-ray guidance under local anaesthetic and sedation.
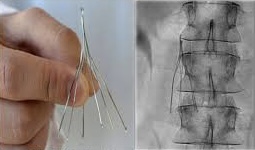
The procedure usually takes approximately 45 minutes. The procedure includes :
After the procedure, you will spend several hours in a recovery room.
Most patients are able to go home the same day. Pain following the procedure is minimal.
Mr Ponosh will not normally see you following the filter insertion or removal as these are very low risk procedures. He will correspond with your referring team and update them with your progress. If the filter needs removal, Mr Ponosh’s rooms, following consultation with your referring team, will organize this procedure.
Of course, if any concerns arise, please contact Mr Ponosh’s rooms, your treating hospital, or your referring team at your earliest convenience.
In almost all cases the filter will be removed as soon as it is not required. This is normally undertaken 2-3 weeks following its insertion. The procedure to remove it is a similar procedure to its insertion. This may be done after your risk of DVT has decreased. The filter should ideally be removed as there can be some long term consequences of prolonged filter placement. Filter removals can be undertaken several months following insertion but this makes the risk of failed removal higher.
In some rare cases, the filter is left in place. This may happen if scar tissue grows around the filter and it cannot be removed or if there is significant clot inside the filter.
All procedures have risks. The risks of this procedure include:
Your risks may vary based on your overall health, the severity of your condition, and other factors. These risks are small and relatively rare.
Click here for a printable Patient Information Sheet on IVC Filters
Click here for a printable Patient Information Sheet on Endovascular Interventions
Click here for a printable Patient Information Sheet on Endovascular Discharge